This web page was produced as an assignment for Genetics 564, an undergraduate course at UW-Madison.
What is Larsen Syndrome?
Larsen Syndrome, first discovered in 1950 by Dr. Loren Larsen, is an rare genetic disorder that occurs in 1 in a 100,000 births (1). Larsen syndrome is passed down through familial generations and in most cases, is autosomal dominant, where only one copy of the affected gene from one parent is needed to express Larsen Syndrome. Though, Larsen Syndrome is sometimes found to be autosomal recessive, where both parents contribute a copy of the affected gene to the offspring (2). The known cause of Larsen Syndrome is missense variants in the DNA coding region (3),of the FLNB (filamin B) gene located on chromosome 3 in the human genome, that leads to the detrimental effects in the development of the bones in those diagnosed with Larsen Syndrome (1). Most reported cases of infants diagnosed with Larsen Syndrome live to become adults and are fertile, but in rare cases this genetic syndrome can be lethal to the fetus during development (4).
What are the common features of Larsen Syndrome?
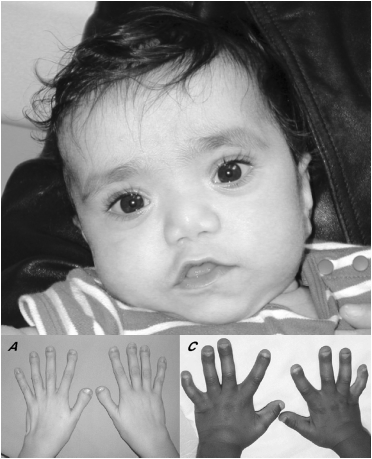
Figure 1: Top: Child diagnosed with Larsen Syndrome showing characteristic facial features of a flat face, depressed nasal passage, wide spread eyes, and low set ears. Bottom: Characteristic spatulate thumbs.
|
Features of those diagnosed with Larsen Syndrome vary in severity, but some common features that appear in most diagnoses are (5): -flat face -depressed nasal passage - prominent forehead - wide spread eyes - low set ears - multiple dislocations: elbows, wrists, hips, knees, ankles (large joints the most common) and can commonly born with dislocations) -short, broad fingers and toes - characteristic spatulate thumbs (squared off) - multiple ossification centers (cartilage formation in bones) -spinal abnormalities such as scoliosis and kyrhosis Uncommon, but recognized features: -hearing loss or impairment (6) - cleft palate (3) -agenesis of the corpus callosum (band of white matter connecting the two hemispheres of the brain fails to connect normally during prenatal development) (7) |
|
|
|
When is a diagnosis made?
|
Most commonly a Larsen Syndrome diagnosis is made after birth, by a medical geneticist and physician team, by a combination of clinical correlation and genetic screening of he FLNB gene. Very few diagnoses have been made prenatally, unless a parent has Larsen Syndrome or if there is suspicion the child would have Larsen Syndrome, such as it running in the family (7). Normally genetic screening is not done prenatally for Larsen Syndrome for it is a rare disorder and the variants involved in Larsen Syndrome have not all been confirmed (8, 9). The few prenatal diagnoses that were made were not able to be absolutely confirmed until after birth for Larsen Syndrome has some similar appearances to other genetic disorders such as Spondylyocarpotarsal syndrome, Atelosteogenesis I and III, and Boomerang Dysplasia (2, 5).
|

Figure 2: Prenatal 3D ultrasound (left) of a the child (right) diagnosed with Larsen Syndrome. Note both dislocated knees and hips. Close monitoring of the child via ultrasound was done in this case for a parent had Larsen Syndrome.
|
What are the known procedures and management associated with Larsen Syndrome?
|
Most patients with Larsen Syndrome have to undergo orthopedic surgery to fix any abnormalities in bone growth or joint dislocations from birth and throughout their life. With these orthopedic surgeries, patients have extensive follow-ups to ensure that everything heals properly as it should and to prevent further extensive surgery. This is because Larsen Syndrome patients take longer to heal and can undergo similar complications that resulted in the original need for surgery (10). Several studies claim that their area of study is the most important area to treat in suffering Larsen Syndrome patients. A briefing of these studies is as follows:
Knee: Dislocation of the knee of a person with Larsen Syndrome has been shown to be one of the most common and difficult areas to treat, as well as one of the first areas to be treated if needed (10). This is because “...most patients are unresponsive to serial manipulation and casting” (10). One case study showed that femoral lengthening of the bone and stretching of the muscle tendons in the leg surgically is a better approach at treating the knee dislocation than serial casting which doesn't work well in Larsen Syndrome patients (11). Though, another study used serial casting and a miniopen quadriceps tenotomy to treat a patient with Larsen Syndrome. Overall, their is some discrepancy on which technique is best in treating knee dislocation in Larsen Syndrome patients, but Larsen Syndrome patients should undergo regular checkups. Neck (Cervical Kyphosis): Cervical kyphosis, a kink in the upper spinal (neck) vertebrate, is thought be the most serious and harmful symptom to treat for patients with Larsen Syndrome because of the risk of life threatening paralysis (12). One study successfully treated one Larsen Syndrome patient with severe cervical kyphosis with a surgical technique known as "posterior arthrodesis", and two other severe patients with "anterior compression and fusion via a lateral approach"(12). In simpler terms, a metal halo loop is surgically placed along the neck vertebrae to correct the severe kink in the patients neck. Any patient with Larsen Syndrome should be screened with a radiograph for cervical kyphosis when they are young to correct the position of the vertebrate of the neck, with minimal invasion, and to prevent paralysis from occurring (12). Spine (Scoliosis): There have been few reported cases of Larsen Syndrome patients having spine issues, specifically scoliosis, but improper spinal alignment or curvature of the spine can occur. Of the few, they can undergo orthopedic surgery as a means to treat their scoliosis (13). One study treated, and greatly improved, a Larsen Syndrome patient by preforming "posterior spinal fusion" from T4 to L2 disks of the spine (about mid-back) (13). The before and after results of said surgery are shown in Figure 4. |

Figure 3: Larsen syndrome child who
underwent orthopedic knee surgery
and is now seen going through orthotic
management.
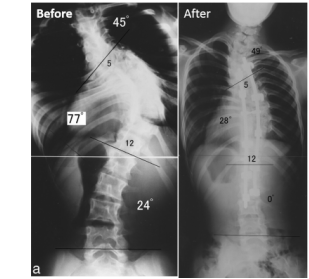
Figure 4: Before and after image of Larsen Syndrome patient who underwent posterior spinal fusion to fix their scoliosis. Adapted figure from (13).
|
Genetic causes of Larsen Syndrome involve the FLNB gene:
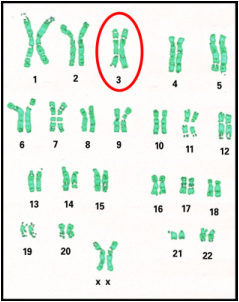
Figure 5: The gene affecting patients with Larsen Syndrome, FLNB, is located on chromosome 3, specifically 3p14.3.
|
Scientists have determined that Larsen Syndrome develops due to missense variants in the FLNB, or filamin B, gene, located of chromosome 3q14.3 (10). The missense variants in the FLNB gene of Larsen Syndrome patients vary, but genetic screening has been performed to determine which variants in the FLNB gene are the cause of Larsen Syndrome. DNA tests done by Zhang et. al, of multiple patients with autosomal and sporadic Larsen Syndrome have shown that “as few as five (of the total of 46) coding exons of FLNB could be screened to detect Larsen Syndrome mutations” (10). Though variants in each patient diagnosed with Larsen Syndrome had distinct variants in their FLNB genes they were able to identify the variants consistent throughout the disorder. By researchers having identified these variant,s and their locations, it is now possible to screen one for Larsen Syndrome through genetic testing by a genetic counselor or other professional geneticist. *More information about the FLNB gene can be found on the "FLNB Gene" page. |
References:
1.) Zhang, D. et. al., (2006) "Mutations Responsible for the Larsen Syndrome Cluster in the FLNB Protein." Journal of Medical Genetics, 43(24), doi: 10.1136/jmg.2005.038695
2.) Gupta, N., and Kabra, M.,"Larsen Syndrome." Indian Pediatrics. 45(9) 2008: 783-4.
3.) Kulkami, M.L., Basha, M.H., Hegade, S., Kumarasamy, T. A., and Kulkami, A. M. "Antenatal Diagnosis of Larsen Syndrome." Indian J Pediatrics. 77(7) 2010:819-20.
4.) Winer, N., et. al., "Prenatal Diagnosis of Larsen Syndrome Caused by a Mutation in the Filamin B gene." Prenatal Diagnosis. 29 (2) (2009): 172-174.
5.) Jones, Kenneth Lyons., David W. Smith, Marilyn Crandall. Jones, and Miguel Del. Campo. "Larsen Syndrome." Smith's Recognizable Patterns of Human Malformation. 7th ed. Philadelphia, PA: Elsevier Saunders, 2013. 564-67. Print.
6.) Stanley, C.S., Thelin, J. W., and Miles, J. H,. "Mixed Hearing Loss in Larsen Syndrome." Clinical Genetics. 33(5) (1988): 395-98.
7.) Shih, E. C., et, al., (2004). "Three-dimensional Ultrasound Diagnosis and Larsen Syndrome with Further Characterization of Neurological Sequelae." Ultrasound in Obstetrics & Gynecology. 24(1): 89-93.
8.) Krakow, D., et. al., (2004). "Mutations in the gene encoding filamin B disrupt vertebral segmentation, joint formation and skeletogenesis". Nature Genetics, 36(4), doi:10.1038/ng1319
9.) Bicknell, L. S., et. al., (2007). "A molecular and clinical study of Larsen Syndrome caused by mutations in FLNB". Journal of Medical Genetics, 44(1), doi:10.1136/jmg.2006.043687
10.) Dobbs, M. B., Boehm, S., Grange, D. K., and Gurnett, C. A., (2007). "Congenital Knee Dislocation in a patient with Larsen Syndrome and a Novel Filamin B Mutation." Clinical Orthopaedics and Related Research. 466(6), doi:10.1007/s11999-008-0196-5
11.) Kaissi, Al., et. al., (2011). "The Management of Knee Dislocation in a child with Larsen Syndrome". Clinics , 66(7), doi: 10.1590/S1807-59322011000700030
12.) Sakaura, H., et. al,. (2007). "Surgical Treatment of Cervical Kyphosis in Larsen Syndrome: Report of 3 Cases and Review of the Literature." Spine, 32(1), doi: 10.1097/01.brs.0000250103.88392.8e
13.) Hosoe, H., et. al., (2006). "Surgical Treatment of Scoliosis in Larsen Syndrome with Bilateral hip Dislocation". Spine, 31(10), doi: 10.1097/01.brs.0000216447.42297.17
Image References:
Header Image: http://fitnessmember.com/fitness-articles/tips-to-stop-knee-pain/
Hand Image: Bicknell, L. S. et. al,. "A Molecular and Clinical Study of Larsen Syndrome Caused by Mutations in FLNB." J Med Genet. 44.2 (2007): 89-98. PubMed. Web. 25 Jan. 2014.
1.) Zhang, D. et. al., (2006) "Mutations Responsible for the Larsen Syndrome Cluster in the FLNB Protein." Journal of Medical Genetics, 43(24), doi: 10.1136/jmg.2005.038695
2.) Gupta, N., and Kabra, M.,"Larsen Syndrome." Indian Pediatrics. 45(9) 2008: 783-4.
3.) Kulkami, M.L., Basha, M.H., Hegade, S., Kumarasamy, T. A., and Kulkami, A. M. "Antenatal Diagnosis of Larsen Syndrome." Indian J Pediatrics. 77(7) 2010:819-20.
4.) Winer, N., et. al., "Prenatal Diagnosis of Larsen Syndrome Caused by a Mutation in the Filamin B gene." Prenatal Diagnosis. 29 (2) (2009): 172-174.
5.) Jones, Kenneth Lyons., David W. Smith, Marilyn Crandall. Jones, and Miguel Del. Campo. "Larsen Syndrome." Smith's Recognizable Patterns of Human Malformation. 7th ed. Philadelphia, PA: Elsevier Saunders, 2013. 564-67. Print.
6.) Stanley, C.S., Thelin, J. W., and Miles, J. H,. "Mixed Hearing Loss in Larsen Syndrome." Clinical Genetics. 33(5) (1988): 395-98.
7.) Shih, E. C., et, al., (2004). "Three-dimensional Ultrasound Diagnosis and Larsen Syndrome with Further Characterization of Neurological Sequelae." Ultrasound in Obstetrics & Gynecology. 24(1): 89-93.
8.) Krakow, D., et. al., (2004). "Mutations in the gene encoding filamin B disrupt vertebral segmentation, joint formation and skeletogenesis". Nature Genetics, 36(4), doi:10.1038/ng1319
9.) Bicknell, L. S., et. al., (2007). "A molecular and clinical study of Larsen Syndrome caused by mutations in FLNB". Journal of Medical Genetics, 44(1), doi:10.1136/jmg.2006.043687
10.) Dobbs, M. B., Boehm, S., Grange, D. K., and Gurnett, C. A., (2007). "Congenital Knee Dislocation in a patient with Larsen Syndrome and a Novel Filamin B Mutation." Clinical Orthopaedics and Related Research. 466(6), doi:10.1007/s11999-008-0196-5
11.) Kaissi, Al., et. al., (2011). "The Management of Knee Dislocation in a child with Larsen Syndrome". Clinics , 66(7), doi: 10.1590/S1807-59322011000700030
12.) Sakaura, H., et. al,. (2007). "Surgical Treatment of Cervical Kyphosis in Larsen Syndrome: Report of 3 Cases and Review of the Literature." Spine, 32(1), doi: 10.1097/01.brs.0000250103.88392.8e
13.) Hosoe, H., et. al., (2006). "Surgical Treatment of Scoliosis in Larsen Syndrome with Bilateral hip Dislocation". Spine, 31(10), doi: 10.1097/01.brs.0000216447.42297.17
Image References:
Header Image: http://fitnessmember.com/fitness-articles/tips-to-stop-knee-pain/
Hand Image: Bicknell, L. S. et. al,. "A Molecular and Clinical Study of Larsen Syndrome Caused by Mutations in FLNB." J Med Genet. 44.2 (2007): 89-98. PubMed. Web. 25 Jan. 2014.
Site Created By: Mary-Kayt Jones
Email: [email protected]
Last Updated 5/19/2014
University of Wisconsin Madison
Genetics 564 Course Page
Email: [email protected]
Last Updated 5/19/2014
University of Wisconsin Madison
Genetics 564 Course Page

{kind=link}